As I've been suffering from knee issues for the last 2-3 years I came to read a lot of stuff regarding knee rehab and health. So I thought trying to make a thread about knee injuries/rehab which is as complete as possible is a good idea, especially as it seems that I'm not the only one that has suffered knee issues in the past. I will write this post down in several parts. Everyone is free to comment, add their own findings etc. The information in this thread is from stuff I read in the internet, the bulletproof knee manual (Mike robertson) and my own findings/observations.
Part 1: Basic knee anatomyAs one is suffering from knee injuries it's essential to know at least the basic things about knee anatomy to fix them.
1.1 Bones of the knee jointThe knee is made up of three main bones
- The Femur (thigh bone) --> above the knee
- The Tibia (shin bone) --> below the knee
- The patella/kneecap --> sits between the patellar ligament and the quadriceps tendon
The thigh bone (femur) meets the large shin bone (tibia) forming the main tibio-femoral joint. The kneecap (patella) joins the femur to form a third joint, called the patellofemoral joint
All of these bony structures are covered in articular cartilage which are designed to decrease the frictional forces as movement occurs between the bones.
 1.2 Passive stabilizing structures
1.2 Passive stabilizing structures- The knee joint capsule --> circulates synovial fluid to the articulating surfaces which reduces friction and "cushions" them
- The Cruciate ligaments (anterior cruciate ligament = ACL/posterior cruciate ligament = PCL) --> cross each other in a X-shaped fashion, they provide anterior and posterior stability within the knee. ACL (anterior stability) provides tibia from moving forward. PCL (posterior stability) prevents tibia from moving backward.
- The collateral ligaments (medial collateral ligament = MCL/lateral collateral ligament = LCL) --> on the outer side of the knee, they provide medial/lateral stability. MCL prevents the knee joint from too much inward movement the LCL from excessive lateral movement.
- The menisci --> between the femur and the tibia there are two crescent shaped rings called the menisci. There is one meniscus on the inside (medial meniscus) and one on the outside (lateral meniscus). The primary role of the meniscus is to promote shock absorbtion at the knee joint.
 1.3 The active stabilizing structures
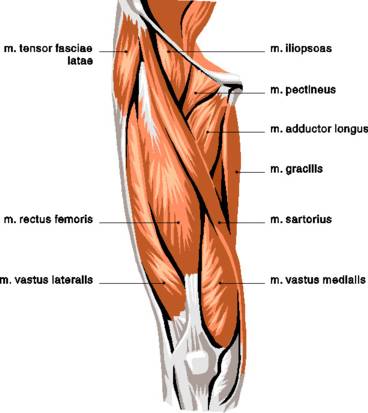
1.3 The active stabilizing structuresThere are several muscles surrounding your knee which provide dynamic stability when moving.
On the anterior side the quadriceps is the main stabilizer --> VMO (vastus medialis oblique; inside), VL (vastus lateralis; outside) rectus femoris (in the "middle")
On the posterior side we have hamstrings, glutes and the calfs
 Part 2: Understanding knee injuries
Part 2: Understanding knee injuriesI don't want to get into much detail on specific knee injuries like ITB syndrom, jumpers knee, patellar tendinitis or whatnot here but just address it in a more general way. Basically there are two types of knee injuries:
1. Acute knee injuries, where there's an actual trauma involved that occurs
instantaneously --> In sports these include mainly ligament and meniscal tears. These injuries can happen without any external influence (non-contact) or based on contact. As it is pretty easy to figure out what the problem is and how to deal with it I wont talk about these injuries in detail here.
2. Injuries that happen
over a longer period of time, where there isn't any actual trauma involved --> With these types of injuries it is often harder to figure out what the cause of the problem is and how to react. The knee hurts although oftentimes there aren't any structures damaged within the knee. The knee itself isn't the main problem here in many cases but rather manifests issues which lie above or below the knee joint itself that have been overlooked for a considerable time. These problems can be (compare Mike Robertson: "Bulletproof knee manual" s. 16-19) :
- Knee alignment: This results in the knees "caving out" (bow-legged/varus malalignment) or vice versa the knees caving in (knock-kneed/valgus malalignment). Varus alignment causes the load-bearing axis to shift to the inside, which puts more stress and force on the medial (inner) compartment of the knee. Valgus alignment shifts the load-bearing axis to the outside, causing increased stress across the lateral (outer) compartment of the knee.

- Suboptimal muscle function and strength: We're talking about insufficient muscle activation, and muscular disbalances here. The goal is to be able to get the right muscles firing at the rigth time and to strengthen the appropriate musculature.
- Poor strength in surrounding musculature: Strengthening the muscles surrounding your knee joint, the active stabilizers (see above), will protect your knees and - if done right - keeps them healthy. It will promote stability and shock absorbtion, taking away the load from you passive stabilizers (the knee joint, ligaments and menisci)
- Poor mobility in adjacent Joints: The knee needs to be stable in order to stay healthy while it is crucial to have enough mobility at the ankle and hip joint (above/below). If the mobility at these two joints is lacking, your body might try and get the missing mobility from elsewhere, the knee joint. This is NOT good and leaves you at a higher risk of injury.
- Excessive tension in surrounding musculature: Shortening in the muscles of your legs/glutes and a lot of scar tissue/trigger points in these areas can definitely lead to knee pain by itself or at least contribute to it.
- Flat out overuse: When you do too much too soon you will eventuall pay for it. So it is very important to keep a close eye on your volume, intensity and frequency and how your body/knee is reacting.
To summ it up, if your knee hurts it doesnt really mean your knee is hurt. So it is important to look at the muscle tissue and the joints above and below the knee joint when addressing knee problems. Doing so will ensure that your actually treating the problem itself rather than just treating the symptoms (knee pain).
Looks like some decent "glute activation" right there

 Part 3: Knee (p)rehab
Part 3: Knee (p)rehabSo after reading part 2 you might ask yourself, what can I do to improve these aspects I mentioned in order to stay/get healthy. Here are a few things you might want to work on to ensure good knee health. I'm really not trying to reinvent the wheel here.
1. Suboptimal muscle function and strength:
1.1 Glute activationProper glute function is important. Not only for athletic developement but also for knee health. In todays society, where sitting a lot is nothing special anymore but the normality a lot of people have bad glute activation and are highly quad dominant. This puts a lot more stress on your knee joint, something we have to prevent.
Exercises to work on glute activation are:
double-leg glute bridges (glute maximus)
<a href="http://www.youtube.com/watch?v=24B9IRHZzTU" target="_blank">http://www.youtube.com/watch?v=24B9IRHZzTU</a>single-leg glute bridges (glute maximus)
<a href="http://www.youtube.com/watch?v=E_coZsl0OLE" target="_blank">http://www.youtube.com/watch?v=E_coZsl0OLE</a>prone glute (glute maximus)
<a href="http://www.youtube.com/watch?v=S4zIh1XEKMA" target="_blank">http://www.youtube.com/watch?v=S4zIh1XEKMA</a>X-band walks (glute medius)
<a href="http://www.youtube.com/watch?v=20wjJAtPLHg" target="_blank">http://www.youtube.com/watch?v=20wjJAtPLHg</a>Miniband walks (glute medius)
<a href="http://www.youtube.com/watch?v=xJxRps8SSQo" target="_blank">http://www.youtube.com/watch?v=xJxRps8SSQo</a>Side Lying clams (glute medius)
<a href="http://www.youtube.com/watch?v=PNSo5ISUN1s" target="_blank">http://www.youtube.com/watch?v=PNSo5ISUN1s</a>If your glute activation is ok and you don't really need to improve it just pick 2-3 of these exercises and do them before your lowerbody workouts during the warmup phase for 1-2 sets. If your glute activation is poor though you should work on it more. 2-3 exercises for 3 sets each, 3 times a week should suffice. I like to work with higher reps of 12-15 or even higher but you could also lower it a bit and go with 10 reps or so if you prefer. Choose whatever exercise you prefer just make sure you do one exercise for the glute maximus (prone glute, single/doulbe leg bridges) and one for the glute medius (x-band walks, mini band walks, side lying clams).
So how do you know if your glute activation is good or bad? That's easy to find out. Just do the prone glute exercise with the hand and your lowerback... now do you feel your glutes turning on before your low back/hams and do you feel a good contraction in your glutes? If not your glute activation is probably subpar and some more work on it wouldn't hurt. You can also tell if your glute activation is good or bad when you look at the soreness the day after heavy squatting. If only your quads are sore and your glutes feel like they haven't been worked at all that's usually a bad sign!
If your glute activation is decent you could go like:
Before Lowerbody workout 1
prone glute 1x12/each side
mini band walks 1x12/each side
Before lowerbody workout 2
single - leg glute bridges 1x12/each
side lying clams 1x12/each
etc.
If you feel that your glute activation needs more work you can add 2-3 sets to all the exercises in the outline above and do each of these little "programms" twice a week, so you would work on your glute activation 4x/week. You might consider starting out with double leg glute bridges in the beginning though.
You can also increase the intensity of the exercises through added band resistance or added weight on the double/single leg glute bridges. In fact weighted single leg glute bridges can also serve as a very good strengthening exercise for the glutes.
huh? fake? cane I see?! (Off topic)

 1.2 Balancing anterior/posterior chain
1.2 Balancing anterior/posterior chainI know it shounds a bit simplistic when some coaches suggest: "If your knee hurts just hit that p-chain and you'll be fine". But it definitely holds some truth. Because when your anterior chain is way bigger/stronger than your glutes/hamstrings are, your movements are all very quad dominant which puts more stress on the knee joint. Strengthening them glutes and hamstrings through adding in some accessory work for your posterior chain is certainly not a bad idea and will take some loading of your knees, especially when you feel that your lacking in this area. Good exercises are as we (hopefully) all know: RDL's, Deadlifts, GHR's, Pull-throughs
If your knees have been aching a bit too much lately you could also shift the focus to your p-chain for a while. Maintaining your quad strength and working on your p-chain a bit more untill your knees are feeling better again. Furhtermore is proper balance between anterior/posterior chain not only interesting in a health aspect but will also ensure adequate athletic developement. Your only as strong as your weakest link! Don't get me wrong, I see that a good pair of strong quads is very important especially for jumping. But backing them up with some good posterior strength/muscle mass is important for health and athletic performance.
How do you know if your quad dominant? There are different ways to see if there is too much quad dominance present. If it's really an issue you can tell very easily
1. Appearance: quads overshadowing hamstrings
2. Strength: Weak hamstrings/glutes vs. strong quads... as in the weightroom
3. Movement: push running when sprinting etc.
1.3 VMO activation/strength
If your suffering from knee pain you should also consider the strength and motor control of your VMO. Because if your lacking in this area this could definitely contribute to your knee problems. Not only does the VMO work as a main knee stabilizer but also has a very important role in helping to keep the patella in the proper groove. The VMO contributes to the medial pull of the patella whilst on the other hand mainly the vastus lateralis muscle and the ITB pull laterally. Think of it as a constant "tug of war" at the patella.
To ensure proper alignment of the patella, you have to make sure that your VMO is firing properly and has sufficient strength. Because if your VMO is weak/inhibited this can be a huge problem for your knee health as it leads to a stronger lateral pull. The lateral structures (vastus lateralis, ITB) now have a tendency to become increasingly dominant in order to keep the patella in control, making the problem even worse.
So, VMO = weak/inhibited and VL/ITB = dominant/tight. What we need to do now is to work on activating that VMO and making it stronger with general strength movements while we try to lengthen and inhibit the lateral side through means like foam rolling, stretching etc.
... more on that topic later
More parts to follow!

